A United Nations Population Fund (UNFPA) report in Kenya shows 378,397 adolescent and teenage pregnancies for girls ages 10-19 between July 2016 and June this year. More specifically, there were 28,932 girls ages 10-14 and 349,465 girls ages 15-19 who became pregnant. The counties with the highest number of teenage pregnancies begin with Narok, where 40 per cent of its teenagers became pregnant. The list goes on to include the counties Homa Bay at 33 per cent, West Pokot at 29 per cent, Tana River at 28 per cent, Nyamira at 28 per cent, Samburu at 26 per cent, and Migori and Kwale both at 24 per cent. Teenage pregnancies have been linked to poverty. Many people believe girls in poverty engage in “transitional” sex to meet basic needs. Others blame “absentee parents” or a lack of parental guidance and exposure to information on the Internet - both which can lead to curiosity and therefore teenage pregnancy. Yet, others even say these...
As a student physical therapist, my future career is primarily to serve individuals with short-term or long-term physical disability. Working with individuals of various forms of physical disability such as those with cerebral palsy, to stroke survivors, to amputees, I have become more aware and appreciative of buildings and spaces that are physically accessible with ramps, elevators, and ADA bathrooms. However, despite my acute awareness of physical accessibility for individuals with disability, accessibility to sexual and reproductive health for this population was not something that crossed my mind until I stumbled on the anecdote by Stella Chiwaka. Chiwaka, born with albinism, was denied contraceptives at a local health center in Malawi and was told by a health provider that “People like you should not have sex”. As a future health provider, I found this discriminatory act appalling. People with disabilities, just as those without disabilities, have the right to make their own choices--including choices regarding their sexuality and sexual health. To...
The sex education I received was decent, by American standards. When I was eight, my female peers and I were ushered to the music room, where we ate our boxed lunches on the floor and learned about the menstrual cycle. I shuddered at the thought of ever bleeding from “down there” and spent the next several years terrified that I would get my first period in public. When I was twelve, my middle school health teacher projected grainy slides of STD-afflicted genitals and explained that pregnancy and childbirth would ruin your life. The class did, however, cover various forms of contraception and a very brief lesson on consent. When a classmate asked if sperm could, like, crawl up your leg, we all laughed at her question while secretly waiting to hear the answer. When I was fifteen, and approaching a time in my life where comprehensive sexuality education might be especially useful, my otherwise progressive high school recommended an online...
Passersby could hardly miss the bright pink stucco building near downtown Jackson, Mississippi in the southern United States. But the unusual color is not all that makes the building unique. The Pink House, as it’s called, is home to the Jackson Women’s Health Organization, the only remaining abortion clinic in the state of Mississippi. With some of the toughest abortion restrictions in the nation, Mississippi is one of 29 states classified as “extremely hostile” to abortion by leading SRHR research organization the Guttmacher Institute. Women currently cannot obtain an abortion after 15 weeks of gestation, the most restrictive ban in the nation. State governor Phil Bryant has repeatedly pledged to make Mississippi “the safest place in American for the unborn child,” joining other lawmakers in a crusade against reproductive freedom. Yet this ostensible commitment to safety is less a compassion toward Mississippi’s children than a powerful political tool. Despite their professed desire to protect women and children, Governor Bryant and Mississippi state legislators...
When people ask how my summer internship is going, I never know what exactly to say. I usually end up blurting out a rapid mix of emotions: “It’s great!” “I love it!” “But it’s also really sad!” “Super depressing day to day, but I care a lot about the work.” “An awesome place to work but a sad field to be working in right now.” I’m interning at the United Nations Foundation in Washington, DC on the Universal Access Project, which convenes donors and advocates working to improve women’s and girls’ access to family planning around the world. Family planning is a fundamental human right and undeniably one of the best investments countries can make towards sustainable development—it can enable girls to stay in school, prevent maternal deaths, improve women’s financial independence and economic productivity, and has even been identified as a top solution to combat climate change. The Duke Center for Global Reproductive Health and other NGOs have reported frequently about...
Content warning: sexual violence Despite rampant criminalization of abortion around the world, the international community tends to agree on one thing: an exception in cases of rape or incest. Even in the United States, where abortion is a hotly debated political issue, a majority of Americans support legalized abortion in cases where the pregnancy was caused by rape or incest. Most people agree that women should not have to be doubly traumatized by being forced to carry a pregnancy conceived through violence. Yet in Myanmar and Bangladesh, Rohingya refugees have little choice but to do just that. Since August 2017, a military campaign of ethnic cleansing in Myanmar’s Rakhine State has forced hundreds of thousands of Rohingya Muslims to flee their homes, causing the fastest growing refugee crisis in the world. As one of many ethnic minorities in Myanmar, the Rohingya numbered nearly one million in early 2017. But the government of Myanmar, a predominantly Buddhist country, refuses to recognize...
This week has seen an onslaught of negative health news from the United States and around the world. Crisis pregnancy centers in the United States are now allowed to withhold legally available medical options, women in Guam no longer have access to abortion services, and we continue to see daily impacts from the reinstatement of the global gag rule and hear reports of lack of access to reproductive health services from women in refugee camps. It’s easy to get depressed from the seemingly impenetrable amount of work that needs to be done to protect the health and human rights of people around the world. But that’s exactly what we need to do. We need to dig deep, understand the depth of the problems, and develop new partnerships and solutions. I’d like to highlight some exciting news from this past week of just that: people digging deep and developing new solutions to positively impact the health and rights of people across the world. Preventing...
Dried henna powder. Animal feces. Bleach. Grain alcohol. The wire coat-hanger. These are some of the many methods women throughout history have used to terminate an unwanted pregnancy. When the safe method for ending a pregnancy--a surgical or medical abortion--is not available, women turn to these alternative techniques, often risking their bodies and lives in the process. Such methods for terminating a pregnancy or inducing a miscarriage are hardly relics of the past. Improvements in contraceptive access, sexual education, women’s empowerment, and abortion access, though significant, have been disparate. In many places around the world, cultural, legal, and financial barriers continue to prevent women from accessing basic healthcare services like contraception and abortion. These obstacles are often magnified in times of crisis. Natural disasters, wars, economic crises, and a host of other factors can all further infringe upon women’s reproductive freedom. Women may lose access to healthcare services, or become uniquely vulnerable to violence. When faced with an unplanned, unwanted,...
If April showers bring May flowers, what do May flowers bring? June rainbows! Each June in the United States, individuals across the nation join in celebrating LGBTQ Pride Month, a time marked by celebration, protest, activism, and, of course, the bright rainbow Pride flag. The tradition was born out of the 1970 Gay Pride March, which took place in New York City to commemorate the Stonewall uprising. As the LGBTQ movement grew, so did Pride marches and within a few years, this form of political protest had spread across the United States, eventually expanding from a single march to a month of events for all LGBTQ people. Over the years, Pride has shifted from primarily a political protest, to a more celebratory occasion. The increasing sociocultural acceptance of LGBTQ people and same-sex relationships has played a role in this shift, and the recent Supreme Court decision in favor of marriage equality is undoubtedly worth celebrating. Yet queer communities certainly remain marginalized...
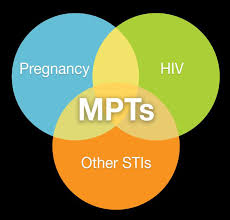
Multi-purpose prevention technologies (MPTs) are the future for female-driven sexually transmitted infection (STI) and unplanned pregnancy prevention. Although dozens of products are in the MPT development pipeline, including several at the final stages of clinical trials, progress in development has been slow, and investment paltry. In my last post, I discussed the technical and scientific barriers that are slowing down MPT research. Today I will highlight the comparable societal barriers, namely: lack of government willpower, widespread poor understanding of the depth and breadth of these health issues, and funding troubles. First, though HIV and unplanned pregnancies receive substantial attention in the fields of global health and development, other STIs tend to be much more overlooked. Fewer global health organizations conduct regular surveillance of non-HIV STIs, preventing more funding from going to their prevention. For instance, the World Health Organization’s (WHO) 2015 Report on global sexually transmitted infection surveillance reported an estimated 357.4 million new infections worldwide (roughly 1 million per...